Diagnosis delay in endometriosis due to posterior compartment misevaluation
Image Description
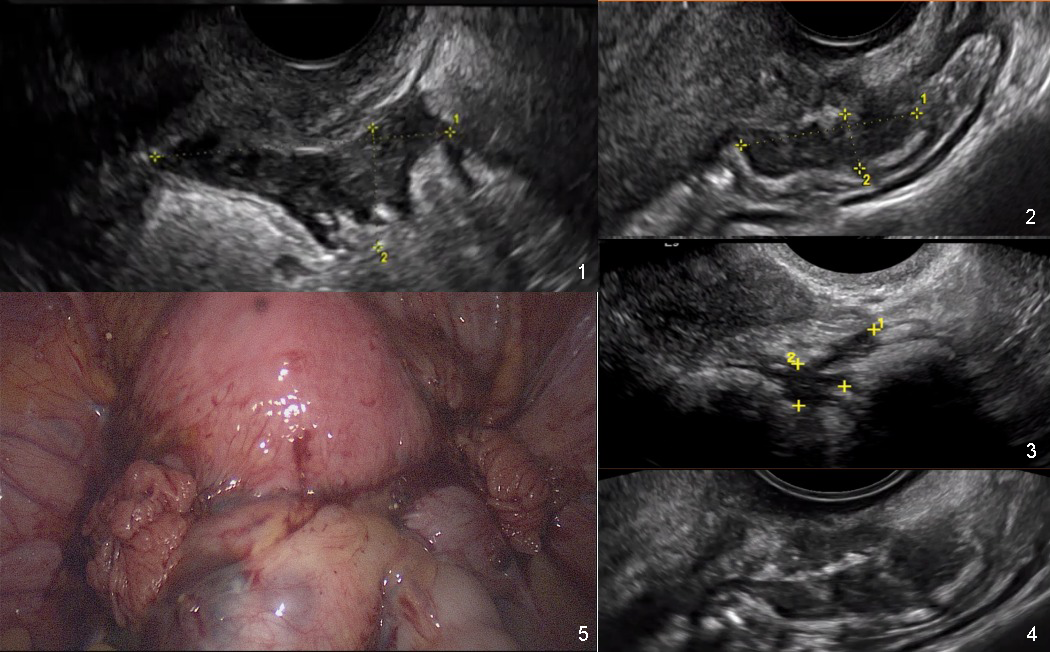
Endometriosis is a complex inflammatory disease that can lead to dysmenorrhea, chronic pelvic pain, dyschezia, dyspareunia, and infertility [1]. The endometrial glands and stroma outside the uterine cavity create a chronic inflammatory milieu that leads to fibrosis, pelvic adhesions, and scarring [2], [3]. If not treated, the adhesions and fibrosis determine frozen pelvis, characterized by distortion of the anatomical structures and fibrosis [4]. Transvaginal ultrasonography (TVUS) and magnetic resonance imaging (MRI) are the most convenient diagnostic methods for endometriosis. Severe stages involve the obliteration of the Pouch of Douglas (POD) through a bowel endometriosis nodule. The sliding sign is a dynamic test used for assessing the POD. It consists in applying gentle pressure with the transvaginal transducer, towards the cervix, to establish if the anterior wall of the rectum glides freely across the retrocervix and posterior vaginal wall. The sliding sign is negative when the organs do not glide freely [5].
We report a case of a 35 years old patient, referred to our clinic with severe chronic pelvic pain, dyschezia, and dyspareunia. The patient had received antibiotics and anti-inflammatory treatments for chronic pelvic pain syndrome for five years. Several doctors affirmed her uterus and adnexa looked ultrasonographically normal. No one had checked the posterior pelvic compartment involving the rectal wall. The large endometriotic nodule on the rectum can be observed in the pictures above (Fig 1-5).
We want to emphasize that it only takes a few seconds to turn the transducer around and discover a possible rectal endometriotic nodule.
References
. Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014 May;10(5):261-75. doi: 10.1038/nrendo.2013.255. Epub 2013 Dec 24. PMID: 24366116.
. Bulun SE, Yilmaz BD, Sison C, Miyazaki K, Bernardi L, Liu S, Kohlmeier A, Yin P, Milad M, Wei J. Endometriosis. Endocr Rev. 2019 Aug 1;40(4):1048-1079. doi: 10.1210/er.2018-00242. PMID: 30994890; PMCID: PMC6693056.
. Nisenblat V, Bossuyt PM, Farquhar C, Johnson N, Hull ML. Imaging modalities for the non-invasive diagnosis of endometriosis. Cochrane Database Syst Rev. 2016;2(2):CD009591. Published 2016 Feb 26. doi:10.1002/14651858.CD009591.pub2
. Working group of ESGE, ESHRE, and WES, Keckstein J, Becker CM, et al. Recommendations for the surgical treatment of endometriosis. Part 2: deep endometriosis. Hum Reprod Open. 2020;2020(1):hoaa002. Published 2020 Feb 12. doi:10.1093/hropen/hoaa002
. Venkatesh S, Anjali M, Vasudeva A, Kumar P. Sliding Sign and Gel Sonovaginography: A Sneak Peek Prior to Laparoscopy in Patients with Endometriosis. J Hum Reprod Sci. 2020;13(1):26-30. doi:10.4103/jhrs.JHRS_169_19