Disseminated cryptococcosis due to Cryptococcus deneoformans in an immunosuppressed patient
Image Description
The prevalence of cryptococcosis in Haematopoietic Stem Cell Transplantation (HSCT) recipients is very low [1]. However, these patients are at a high risk of life-threatening complications due to immunosuppressive therapy. The coexistence of Graft-versus-Host Disease (GvHD) further complicates management [2]. Skin involvement in cryptococcosis is rare and an early marker for disseminated disease. Cryptococcus deneoformans rarely causes disease [1].
A 71-year-old male patient was admitted to the Emergency Department with a 15-day history of inflammatory signs on his left forearm, without improvement on oral flucloxacillin and piperacillin-tazobactam. His past medical history was significant for T-cell lymphoma, in remission after Allo-HSCT in 2014, and coexistent chronic GvHD under ruxolitinib. On hospitalization day 4, the soft tissue infection worsened, characterized by drainage of purulent exudate. This was collected and sent for bacteriological and mycological studies.
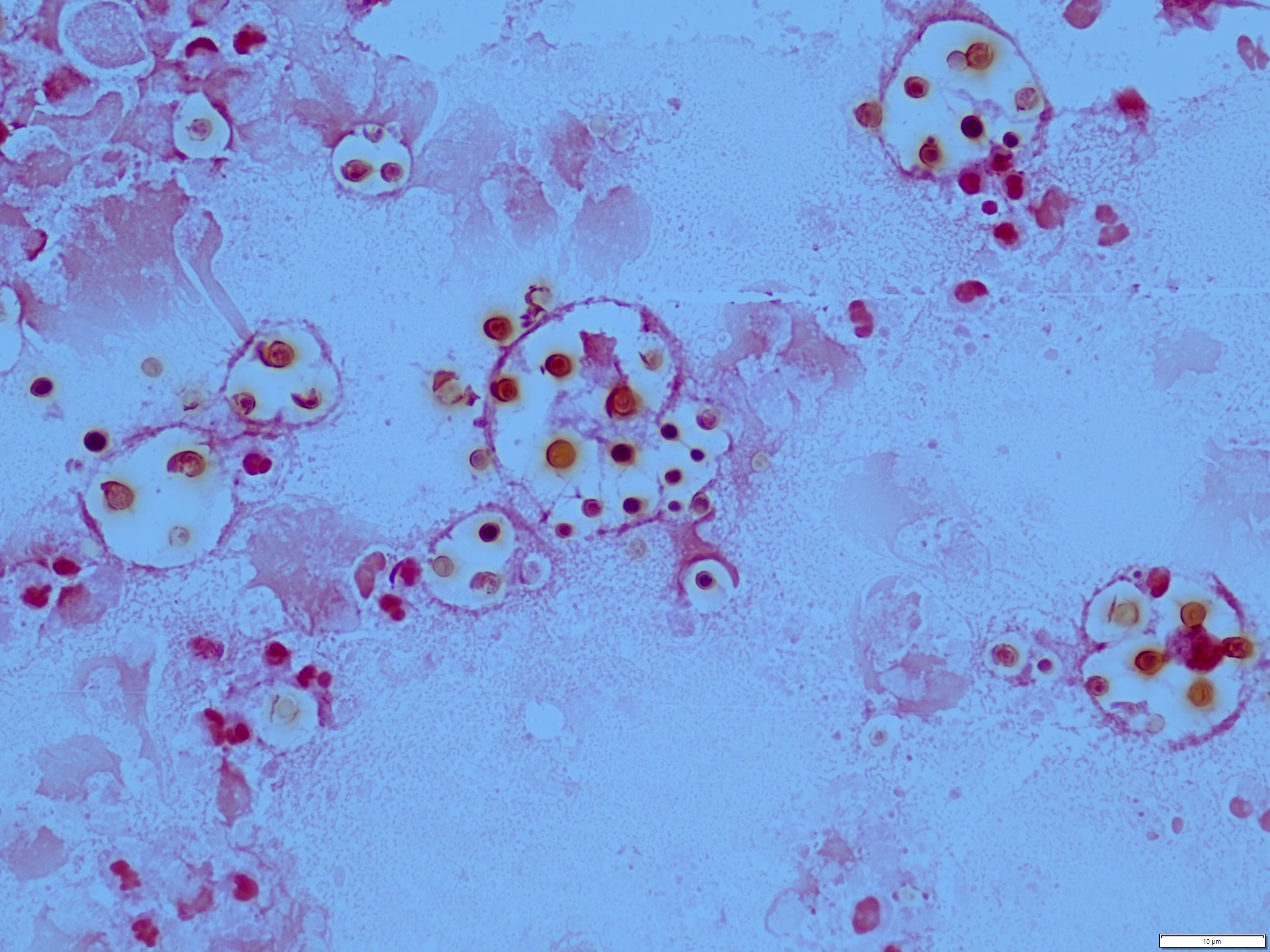
In the laboratory, direct microscopic examination of the exudate revealed small, round yeast forms (Figure 1), surrounded by a clear halo which did not stain with the Gram method, raising suspicion for Cryptococcus spp. When the exudate was prepared with India ink, it highlighted the encapsulated yeast. This finding was consistent with a diagnosis of cryptococcosis and liposomal amphotericin B was initiated. Cultures grown from the sample showed white, smooth colonies within 18-24 hours of incubation. These colonies were identified as Cryptococcus deneoformans by MALDI-TOF mass spectrometry. Subsequent blood cultures were also positive for C. deneoformans, confirming the diagnosis of disseminated cryptococcosis. The patient underwent 45 days of liposomal amphotericin B, with gradually improving clinical condition.
References
Nematollahi S, Dioverti‐Prono V. Cryptococcal infection in haematologic malignancies and haematopoietic stem cell transplantation. Mycoses. 2020; https://doi.org/10.1111/myc.13153
Firacative C, Carvajal SK, Escandón P, Lizarazo J. Cryptococcosis in Hematopoietic Stem Cell Transplant Recipients: A Rare Presentation Warranting Recognition. Can. J. Infect. Dis. Med. Microbiol. 2020; https://doi.org/10.1155%2F2020%2F3713241